


 CC-BY 4.0
CC-BY 4.0
1. Introduction
Nephrolithiasis is a frequent urologic diseases affecting more than 10% of the population, with a peak of incidence between 40 and 60 years [1, 2]. Combining with a high percentage of recurrence, from 40% to 50% within ten years [3, 4], this pathology has particular social and economic implications [5]. While some genetic predispositions lead to particular type of stones, life and dietary habits largely contribute to renal stone formation (review in [6, 7]). Identifying the nephrolithiasis risk factors that are sometimes specific to a region or a country is of particular interest for the patients’ treatment. In Switzerland there is ongoing research to improve the understanding of nephrolithiasis (Swiss Kidney Stone Cohort) [8], but until now, few epidemiological data are available on the demographic information of Swiss patients suffering from this pathology as well as on the composition of their calculi. The Laboratory of Biological Fluids at the Geneva University Hospitals in Switzerland receives for analysis calculi from a large part of the west of the country. The objective of this study was to take advantage of our database containing the results of 10,437 stone analyses gathered between 2009 and 2019 to investigate a possible association of gender and age with calculi composition, determine any emerging trends in stone formation, and draw a picture of nephrolithiasis in the Romandie part of Switzerland.
2. Methods
The Laboratory of Biological Fluids at the Geneva University Hospitals processes analysis of calculi received from Geneva, Vaud, Neuchatel and Valais cantons that are located in the Romandie part of Switzerland. Request analyses were received from either independent private laboratories or hospitals such as the University Hospitals of Lausanne or Geneva. A retrospective review was performed of all stones examined in our laboratory from the years 2009 to 2019. Starting from a database of 10,609 calculi collected, a total of 10,437 renal stones were selected and associated with patient’s demographic information such as age and sex. These calculi were obtained by spontaneous passage, ureteroscopy, percutaneous nephrolithotomy or shockwave lithotripsy.
Stone composition was determined by morphologic examination combined with Fourier-Transformed infrared (FTIR) spectroscopy. More precisely, FTIR analysis was performed on powdered samples of the different parts of each stone by Spectrum 100 from Perkin Elmer Life (Shelton, USA) combined with an ATR accessory (Specac, Orpington, UK). The spectra were collected in the 4000–540 cm−1 mid infrared range at a resolution of 4 cm−1 with eight scans. Each spectrum was analysed by the Spectrum software (Perkin Elmer Life, Shelton, USA) and the proportion of each component was assessed. Minor components accounting for less than 5% (e.g. proteins and mucopolysaccharides) of the stone were neglected except carbapatite in Randall’s plaque.
The data were analysed with GraphPad prism software using the Mann–Whitney test for comparison of age, and Chi-squared test for comparison of frequencies. Results with p value < 0.05 were considered as statistically significant.
3. Results
3.1. Overall picture
Between 2009 and 2019, 10,437 renal stone analyses were performed in our laboratory. The number of analysed calculi steadily increased, starting from 461 stones/year in 2009 to 1393 stones/year in 2019 (3-fold increase; Figure 1A). The male-to-female gender ratio was in favour of men (average of 2.49 ± 0.17), constant along the years and both gender contributed equally to the observed increase in the number of calculi (3.05-fold increase for women and 3.0 for men; not shown). The mean age at stone episode was 50.6 ± 11.3 years, and the difference between men and women age was statistically significant (52.3 ± 15.9 years for men and 49.8 ± 17.2 years for women (p < 0.0001)). Overall, the majority of patients had 41 to 60 years at stone episode (45%; Figure 1B), 26.1% had 61 to 80 years, and 20.4% had 26 to 40 years. Children ages 0 to 15 showed the lowest incidence of stone formation (1% of calculi), and patients aged 16 to 25 or above 80 years accounted for 4 and 3.8% of calculi, respectively.
Stones from 2009 to 2019. (A) Number of stones by year of analysis and gender. (B) Repartition of stone episode by patient age groups. (C) Frequency of stones composed by 1, 2, 3 or more (4 or 5) components. (D) Frequency of calcium oxalates, calcium phosphates, uric acids (anhydrous uric acid and/or uric acid dihydrate), or other components (urates, struvite, cysteine, proteins, drugs) presence in all stones.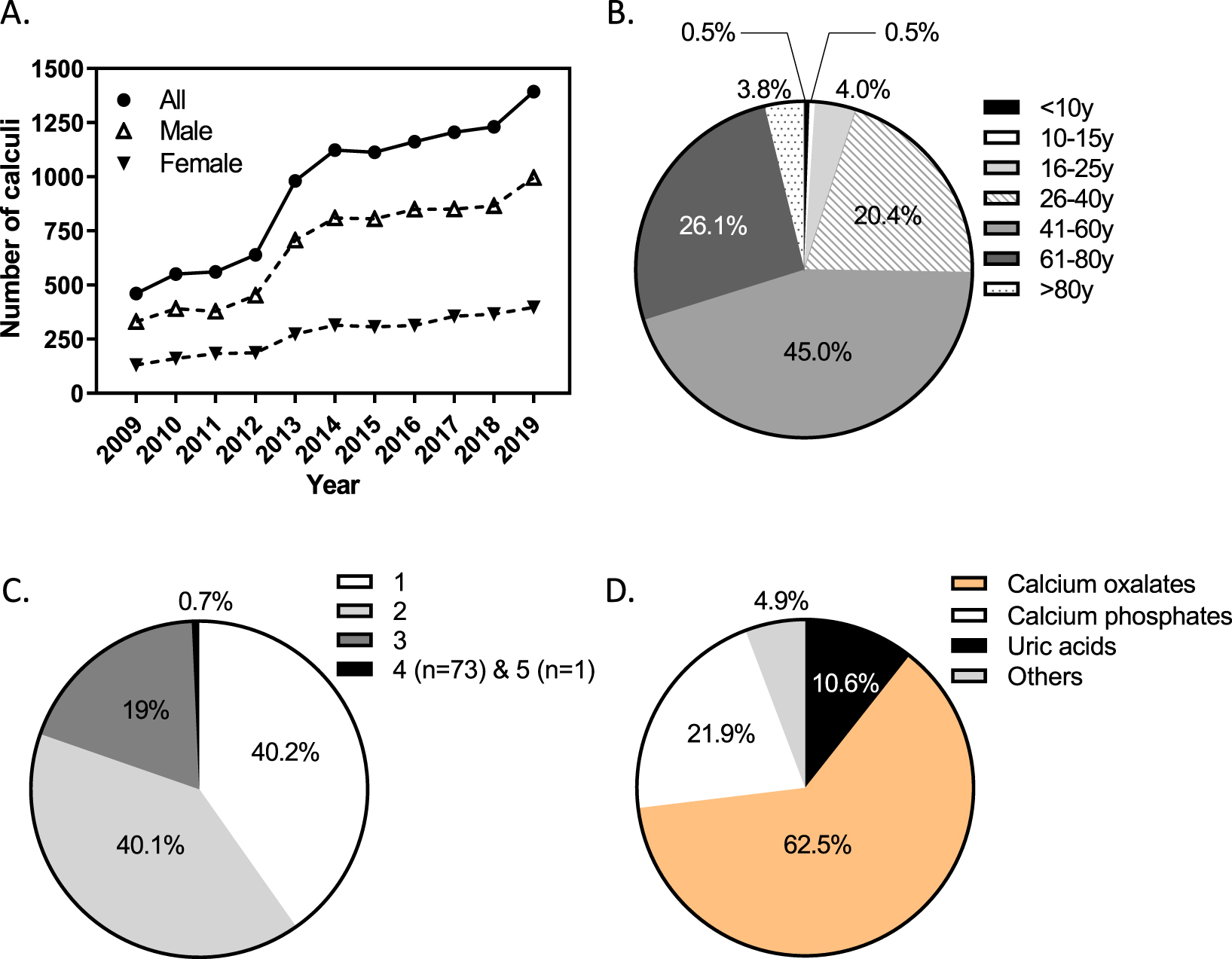
The analysis of the 10,437 stones by morphological characterization and FTIR spectroscopy revealed the presence of 18,804 compounds. The majority of calculi were composed of one or two compounds (40.2% and 40.1%, respectively), but we identified at least three or more compounds in 19.7% of stones (Figure 1C). Calcium oxalates were the most frequent compounds (62.5%, Figure 1D), followed by calcium phosphates (21.9%) and uric acids (10.6%). Other identified compounds (4.9%) were urates, struvite, cystine, drugs and proteins.
3.2. Stone composition
3.2.1. Calcium oxalate stones
Calcium oxalate monohydrate (COM) was the most represented compound and found in 78.1% of stones, with a mean age of patients of 51.2 years (Table 1). Except for children below ten years, it was the most frequent compound in calculi whatever the gender and patient age (Table 1 and Figure 2). The mean age of women experiencing COM stones was significantly lower than that of men (49.5 versus 51.9 years, p < 0.0001).
Calcium oxalate dihydrate (COD) was less frequent and found in 34.4% of stones. It accounted for more than 50% of the stone in 11% of cases, with a significant higher frequency for men (11.8%) than women (8.9%, p < 0.001). The mean age of patients was younger (46.2 years) than for COM, regardless of sex (Table 1). In line with that, the highest COD frequency was observed for men aged 16–25 years and the presence of this compound in male stones appeared to increase between the age below ten years and 25 years before decreasing with age (Figure 2). In women, COD frequency peaked at age 10–15 years and lowered thereafter.
3.2.2. Carbapatite stones
Carbapatite was globally the second most frequent compound (38.1% of stones). It was mainly a minor compound, especially in men (Table 1), probably because it was the most frequent constituent of the Randall’s plaque found on some calcium oxalate stones and in such cases, amounted for less than 5% of the stone. Carbapatite was the second most frequent component in adult women (Table 1 and Figure 2A) with a frequency of 51.6%, significantly higher than in men (32.7%) for whom it ranked only at the third place, after calcium oxalates. The lowest frequency was observed in girls aged 10–15 years, and in men it tended to decline with age as for COD (Figure 2).
Distribution of urinary stones by composition
| Compound | All | Women | Men | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total number | Frequency (%) | Age (mean, y) | Frequency as main component (%) (n) | Number | Frequency (%) | Age (mean ± SD, y) | Frequency as main component (%) (n) | Number | Frequency (%) | Age (mean ± SD, y) | Frequency as main component (%) (n) | |||
| COM | 8152 | 78.1 | 51.2 | 61.0 (6366) | 2364 | 79.0 | 49.5 ± 16.5 | 58.4 (1747) | 5788 | 77.7 | 51.9 ± 15.0∗∗∗∗ | 62 (4619) | ||
| Carbapatite | 3978 | 38.1 | 47.6 | 11.1 (1162) | 1543 | 51.6 | 47.6 ± 16.7 | 20.2 (603) | 2435 | 32.7∗∗∗∗ | 47.6 ± 16.2 | 7.5 (559)∗∗∗∗ | ||
| COD | 3589 | 34.4 | 46.2 | 11.0 (1149) | 1016 | 34.0 | 46.7 ± 17.2 | 8.9 (267) | 2573 | 34.6 | 46.0 ± 14.5 | 11.8 (882)∗∗∗ | ||
| UA0 | 1413 | 13.5 | 61.7 | 10.5 (1094) | 220 | 9.6 | 63.3 ± 13.9 | 5.3 (160) | 1193 | 16.0∗∗∗∗ | 61.4 ± 13.2∗ | 12.5 (934)∗∗∗∗ | ||
| UA2 | 585 | 5.6 | 59.9 | 1.1 (118) | 93 | 3.1 | 63.9 ± 13.5 | 0.5 (16) | 492 | 6.6∗∗∗∗ | 59.2 ± 13.0∗∗ | 1.4 (102)∗∗∗ | ||
| STR | 290 | 2.8 | 55.9 | 2.0 (212) | 133 | 4.4 | 51.2 ± 21.4 | 3.3 (99) | 157 | 2.1∗∗∗∗ | 59.9 ± 21.9∗∗∗ | 1.5 (113)∗∗∗∗ | ||
| BR | 104 | 1.0 | 47.0 | 0.7 (76) | 17 | 0.6 | 39.5 ± 14.1 | 0.5 (14) | 87 | 1.2∗∗ | 48.5 ± 14.5∗ | 0.8 (62)∗ | ||
| UAM | 94 | 0.9 | 49.2 | 0.4 (37) | 32 | 1.1 | 46.6 ± 23.5 | 0.3 (8) | 62 | 0.8 | 50.5 ± 28.3 | 0.4 (29) | ||
| UAS | 67 | 0.6 | 54 | 0.1 (14) | 8 | 0.3 | 70.1 ± 14.6 | 0.1 (4) | 59 | 0.8∗∗ | 51.8 ± 14.3∗∗ | 0.1 (10) | ||
| Cystine | 62 | 0.6 | 45.9 | 0.6 (62) | 23 | 0.8 | 49.9 ± 19.5 | 0.8 (23) | 39 | 0.5 | 43.6 ± 11.6 | 0.5 (39) | ||
| Drugs | 15 | 0.1 | 55.5 | 0.1 (11) | 2 | 0.07 | 66.5 ± 30.4 | 0.1 (2) | 13 | 0.2 | 39 ± 12.0 | 0.1 (9) | ||
COM: calcium oxalate monohydrate, COD: calcium oxalate dihydrate, UA0: anhydrous uric acid, UA2: uric acid dihydrate, STR: struvite, BR: brushite, UAM: ammonium hydrogen urate, UAS: sodium hydrogen urate, CYS: cysteine, Drugs: stones containing amoxicillin, atazanavir or 5-aminosalicyclic acid. Frequency (%): percentage of stones containing the compound. Frequency as main component: number of times (%) a component accounted for more than 50% of the stone in the whole series of 10,437 calculi. Comparison between men and women is statistically significant with ∗∗∗∗ p < 0.0001, ∗∗∗ p < 0.001, ∗∗ p < 0.01, ∗ p < 0.05 (Mann–Whitney test for comparison of age and Chi-squared test for comparison of frequencies).
Component frequency by age groups and gender between 2009 and 2019.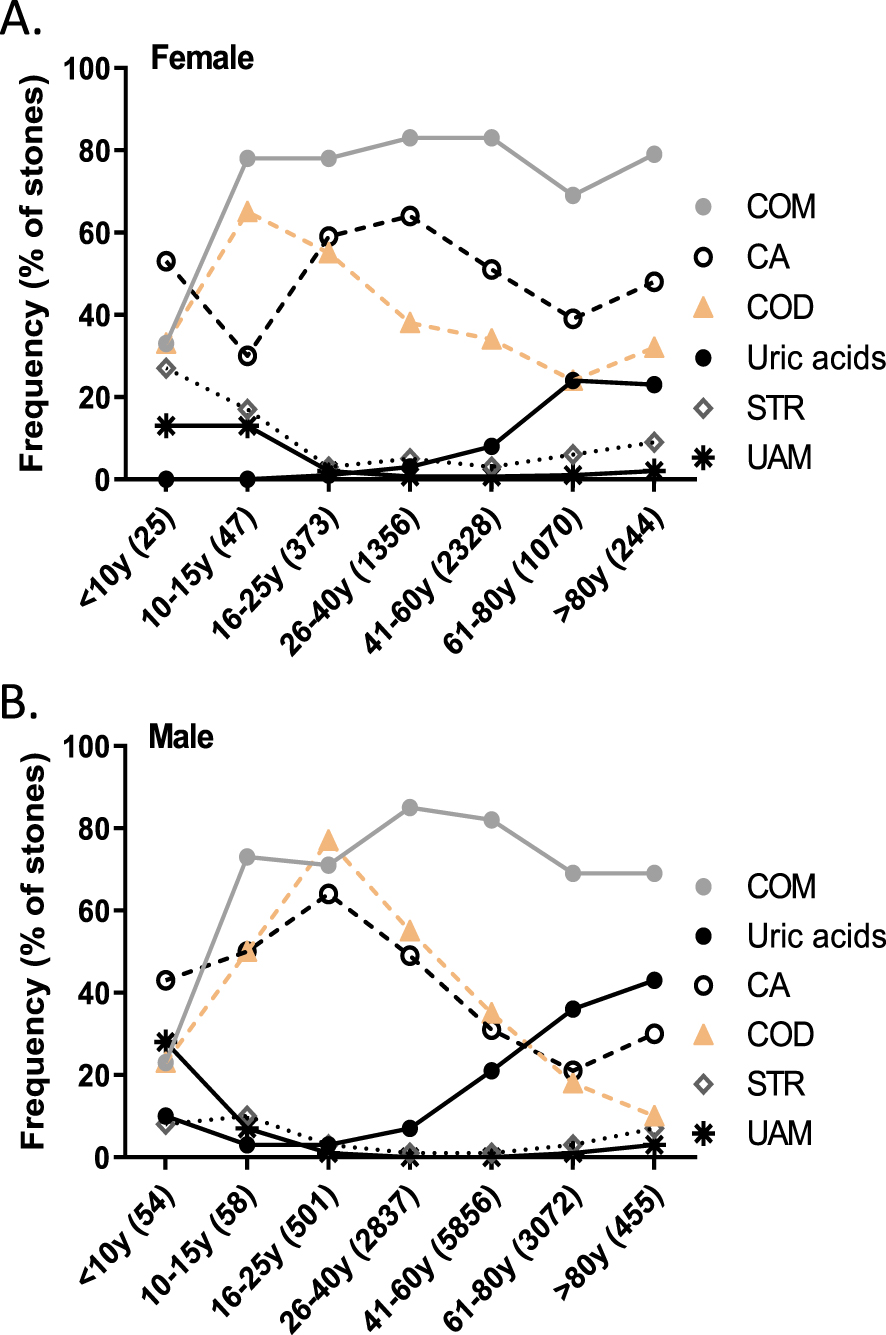
3.2.3. Uric acid stones
Uric acids held the fourth place in compound frequency for both gender, reaching 13.5% for anhydrous uric acid (AU0) and 5.6% for uric acid dihydrate (AU2), with a mean age of patients of 61.7 and 59.9 years, respectively, which are the highest observed in our study (Table 1). Both type of uric acids were about twice more frequent for men than women (p < 0.0001, Table 1) and when it accounted for more than 50% of the stone, AU0 was the second most frequent compound for men (11% of cases) but only the fourth for women (5.3%, p < 0.0001), the latter being older when experiencing such calculi (p < 0.05 for AU0, and p < 0.01 for AU2). Finally, the number of uric acid stones increased with age, from the fourth decade in men but only from the sixth decade in women (Figure 2).
3.2.4. Struvite stones
Struvite (magnesium ammonium phosphate hexahydrate) was identified in 290 calculi (2.8% of stones; Table 1). More women than men experienced struvite calculi (4.4% and 2.1%, respectively, Table 1), with a frequency as main component also statistically different between gender (3.3% for women and 1.5% for men, p < 0.0001). The mean age of patient was also lower for women (51.2 versus 59.9 years, respectively; p < 0.001), and this was partly due to the age groups below 15 years who had the highest number of struvite calculi (Figure 2A).
3.2.5. Brushite stones
Brushite (dicalcium phosphate dihydrate) was identified in 104 stones (1.0% of stones; Table 1), more for men than women (1.2% and 0.6%, respectively, Table 1). The difference in the mean age of both gender (39.5 years for women and 48.5 for men) was statistically significant (p < 0.05).
3.2.6. Other components
Ammonium hydrogen or sodium hydrogen urates were present in 0.9 and 0.6% of calculi, respectively (Table 1), with a higher prevalence in younger men for the latter (p < 0.01, Table 1). Surprisingly, ammonium hydrogen urate was the second compound found for boys below 10 years, after calcium oxalate monohydrate, whereas it ranked at the fifth place for girls, after calcium oxalates and struvite (Figure 2).
Cystine calculi were rare: 62 from 35 patients in ten years, with a mean age of 45.9, higher in women than in men (49.9 versus 43.6 years). Cystine was the major compound in all cases.
Finally, we identified 15 stones made up of the drug atazanavir (n = 13, 11 patients, 1 woman and 10 men), amoxicillin (1 woman), or mesalazine (5-aminosalicylic acid, 1 man) crystals. No 2,8-dihydroxyadenine stone was detected.
3.3. Evolution of age at stone episode
For children below 15 years, the number of analysed calculi remained unchanged and low along the years (Figure 3). No clear evolution was observed between 2009 and 2019 for both gender at age 16–25. For men and women, the highest increase of number of stone analysed was observed for patients aged from 41 to 60 years old (about 4-fold). This age group accounted for about half of the stones per year for men regardless of the year. Male patients of 26–40 and 61–80 years had also an increase in number of calculi, which was stronger for the latter (Figure 3B). On the contrary, the tendency of increase in stone numbers was similar for the same age groups in women (Figure 3A), but the proportion of stones for the 26–40 group age was higher than for men. Finally, all patients aged over 80 years showed also an increasing trend to have more stone episodes.
Number of stones by age groups and year of analysis.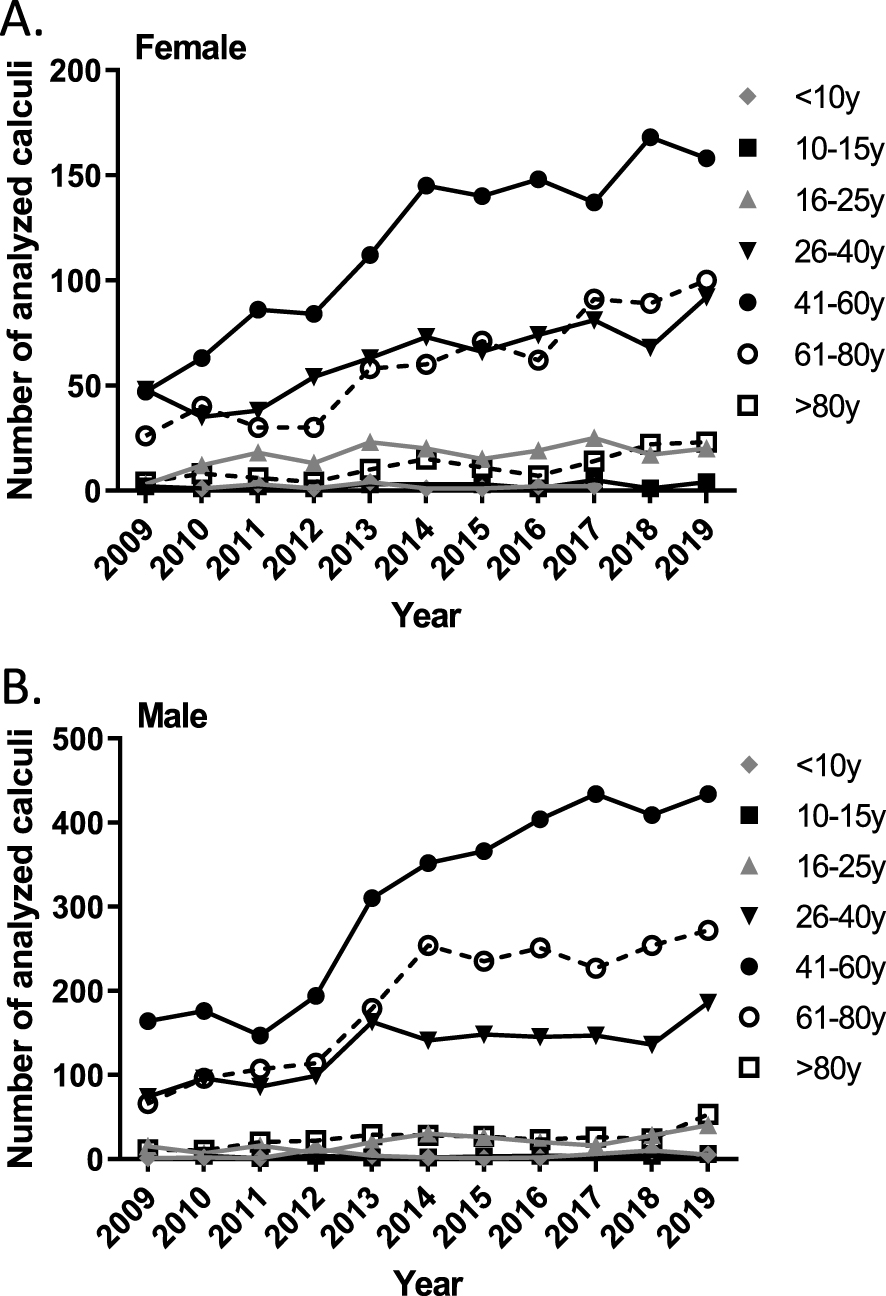
3.4. Evolution of stone composition
Overall no trends regarding a change in compound frequency were observed along the ten years (Figure 4), except for COD whose frequency increased along the years, particularly in women (23.1% to 47.4%; Figure 4A). Carbapatite frequency did not change, being always higher for women (Figure 4B). Anhydrous and dihydrate uric acids showed no clear tendency whatever the sex but were every year higher in men than in women (Figure 4C). Finally presence of struvite did not change along the years and was in general more frequent in women (Figure 4D).
Evolution with time of component frequency by gender. F, female; M, male.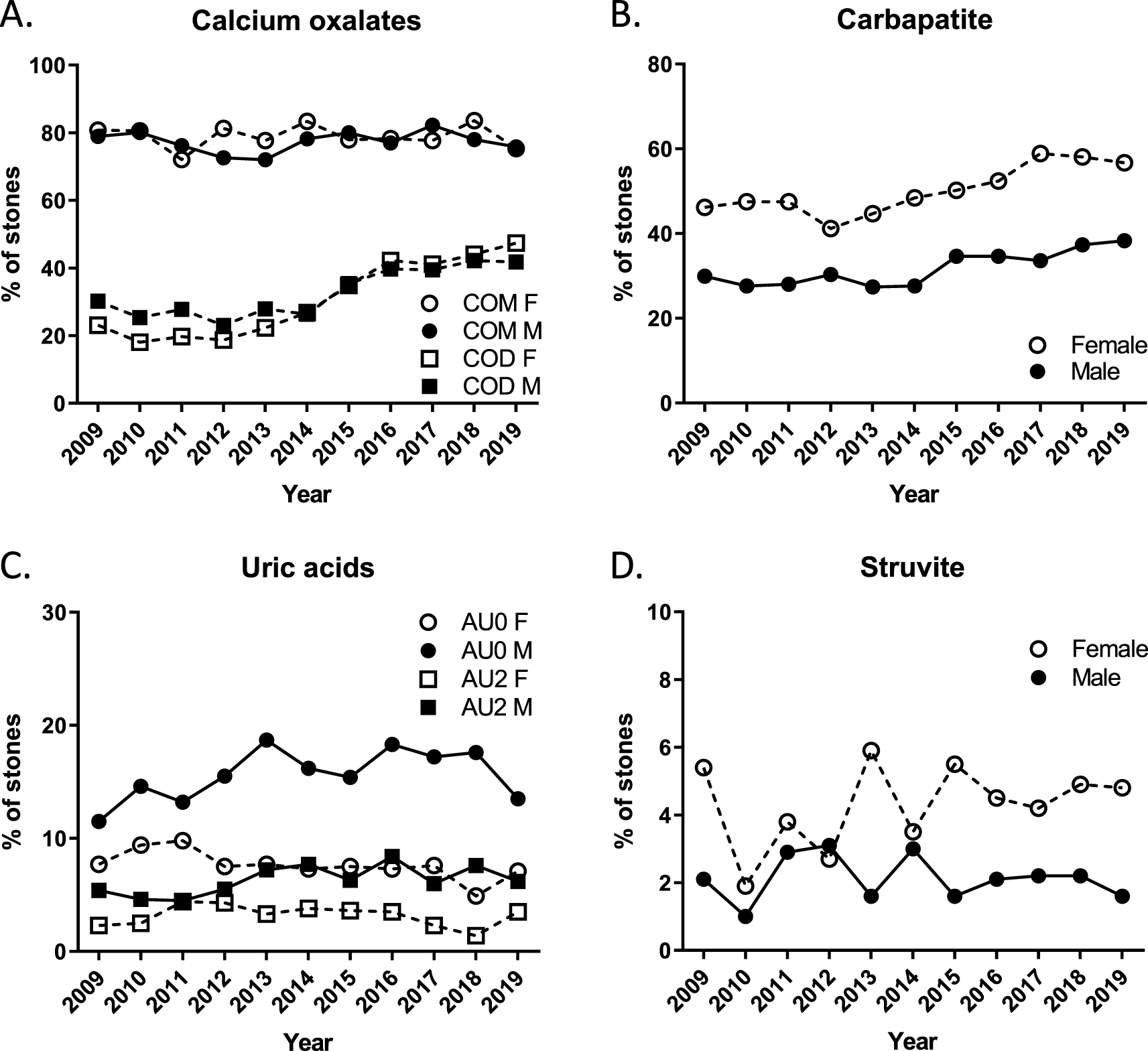
Among the less common components, brushite had an increasing trend during the period of 2009 to 2019, especially in women (0% in 2009 to 1.3% in 2019, data not shown).
3.5. Presence of Randall’s plaque on calcium oxalate stones
Randall’s plaque (RP) is a calcium phosphate deposit at the tip of the renal papilla, considered to be at the origin of calcium oxalate stones [9]. In our laboratory, they were characterized or described only since 2015. Frequency of RP on 4829 COM-containing calculi was 7.4% irrespective of gender (Table 2). The composition of RP determined by FTIR was carbapatite in 86%, sodium urate in 6% and mixed in 1% of cases. In 7% of RP, the crystalline phase could not be identified. Only men had sodium urate in Randall’s plaque (data not shown). Patients with RP were significantly younger (mean age of 45.8 versus 52.4 years, p < 0.0001), and this was not influenced by sex. The age group of 26 to 40 years appeared to have the highest prevalence of RP, whereas children and patients over 60 years had the lowest number of stones with RP.
4. Discussion
Environmental factors account for a large part in the development of nephrolithiasis, making epidemiological studies of particular interest to identify means of action to decrease incidence and prevalence of this disease. This descriptive and retrospective study tried to enhance the understanding of the trend over ten years regarding the chemical components of urinary tract stones. It provides the largest series of stone analyses in Switzerland, with 18,804 compounds identified in 10,437 calculi from patients living in the west and French-speaking part of the country and gathered between 2009 and 2019. To our knowledge, no comparable series has yet been described in this country.
4.1. Stone numbers
The number of stones analysed has grown annually. However such a 3-fold increase in ten years cannot be explained only by a higher incidence and is also probably due to a rise in the number of sources submitting stone analyses to our laboratory.
4.2. Age
Analysed stones were from patients with a mean age of 50.6 years. Patients who experienced the highest number of stones were between 41 and 60 years of age. These results are similar to those described in some studies from other countries [10, 11, 12, 13, 14].
4.3. Sex
The overall male-to-female ratio was 2.49:1 and remained stable over the ten years. This proportion is between the one observed in France (2.1:1; [15]) and in Germany (2.7:1; [16]), two neighbouring countries, but largely different from the one measured in the United States (1.37:1 or 1.55:1, [17, 18]).
Prevalence of Randall’s plaque among calcium oxalate monohydrate stones
| Randall’s plaque | All | Female | Male | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Presence | Absence | % of RP | Presence | Absence | % of RP | Presence | Absence | % of RP | |||
| Total number of COM stones | 358 | 4471 | 7.4% | 98 | 1274 | 7.1% | 260 | 3197 | 7.5% | ||
| Age (years) mean ±SD | 45.8 ±13.0 | 52.4 ±15.5∗∗∗∗ | 43.4 ±12.5 | 51.1 ±16.6∗∗∗∗ | 46.6 ±13.1 | 52.9 ±15.1∗∗∗∗ | |||||
| <15 years | 1 | 30 | 3.2% | 0 | 14 | 0% | 1 | 16 | 5.9% | ||
| 16–25 years | 15 | 143 | 9.4% | 7 | 59 | 10.6% | 8 | 84 | 8.7% | ||
| 26–40 years | 114 | 819 | 12.2%**** | 35 | 268 | 11.6%* | 79 | 551 | 12.5%**** | ||
| 41–60 years | 182 | 2148 | 7.8% | 51 | 578 | 7.7% | 131 | 1570 | 8.1% | ||
| >60 years | 46 | 1329 | 3.4% | 5 | 353 | 1.4% | 41 | 976 | 4.0% | ||
RP: Randall’s plaque. Comparison of mean age between presence and absence of RP is statistically significant with ∗∗∗∗ p < 0.0001 (Mann–Whitney test). Comparison of % of RP between the 26–40 years age group and the overall frequency of RP is statistically significant with ∗∗∗∗ p < 0.0001 for the All and Male groups and ∗ p < 0.05 for the Female group (Chi-squared test).
4.4. Chemical components
In our study, the most frequent component was COM with a frequency of 78.1% followed by carbapatite (38.1%), COD (34.4%) and uric acids (19.1%). Others crystalline phases such as struvite, brushite, and urates showed a frequency below 10%. Considering components present as major compound ( >50% of the stone), the highest frequency was observed for COM, carbapatite, COD and AU0. These proportions were comparable to those described for other countries [10, 15]. Calcium oxalates are the most frequent compounds found in a broad majority of calculi around the world [19]. In our study, their predominance was similar to what has been observed in France. However, in our case, frequency of monohydrate calcium oxalate when present as the main component was similar for both gender, whereas French men had more stones with large amount of COM than French women [15, 19]. For COD, despite an overall frequency as main component lower than in France, we also observed a statistically difference between gender, men having more calculi with COD as the major compound. Although COM-containing calculi were the most common for both gender, women’s stones contained more often carbapatite (51.6% versus 32.7% for men). This ranking was found similar in other countries [13, 15, 17, 19].
A gradual increase in frequency of uric acid stones has been observed for the recent years in different countries [6, 11, 14, 18]. This progression seems to be due to the increase of obesity and type 2 diabetes mellitus associated with a higher susceptibility of women to develop nephrolithiasis in those cases. As in France [15], our results indicates that uric acid containing-stones rank at the fourth place in terms of number for both men and women. Their frequency also increases with age, men experiencing about twice more uric acid calculi than women [19]. In Germany, a study from 2011 put uric acid at the second most common composition in each gender [16]. In our case, the frequency of anhydrous uric acid as main component ranked at the second place but only for men. It would then be interesting to compare our results from the western and French-speaking part of Switzerland to the incidence of uric acid stones in the German-speaking part of the country.
Struvite-containing stones were less frequent in our study (2.8%) compared to others in France (4.5% [15]), in the United States (3.7% for men, 3.0% for women, [18]), but at a similar rate to the one observed in China (3%, [13]). When considering the frequency of struvite as main component, we observed a two-fold difference between women and men (3.3% versus 1.5%, respectively), which was close to the results of Daudon et al. [15] (2.3% versus 1.1%, respectively). As in Yang et al. [13], our data showed that girls below 15 years had the highest number of struvite stones illustrating the higher prevalence of urinary tract infection for this age group.
Finally, cystine frequency (0.6%) was similar to that in other countries such as France (0.9%, [15]), Germany (0.6%, [16]), China (1.1%, [12]; 0.6%, [13]), and the United States (0.4%, [18]).
4.5. Time-related evolution of components
Within the most frequent compounds, we did not observe any evolution over the ten years except an increase for COD frequency (23.1% to 47.4%). A gradual frequency rise of uric acid stones [6, 11, 14, 18] was not found in our series. For these latter components, our results did not show any clear growing trend along the ten years studied as reported in a German study from 1977 to 2006 [16]. Again a comparison of our data with the incidence of uric acid stones in the German-speaking part of the country would be of interest. However, conclusion concerning uric acid stones must be made with great caution as they are the best candidate for stone dissolution by medical treatment after identification by dual-energy computed tomography, which probably leads to an underestimation of their frequency in the laboratory cohort.
4.6. Age-related evolution of components
Influence of age on stone composition has been known for many years. As observed in many studies, mean age of patients experiencing stones of cystine, COD, carbapatite, brushite and ammonium hydrogen urate were under 50. Conversely, the oldest patients had more uric acids as major component of their stones, which is consistent with previous observations showing a rising number of UA calculi with age [14, 16, 17, 19]. Finally, COM was the major component in each age group except for children younger than ten years, for whom carbapatite was the predominant component and accounted for 30% of all stones for each gender.
Uric acids showed a significant increase of 20% in oldest patients while COD decreased in the same proportion for the same age groups. Infectious components such as struvite and ammonium hydrogen urate were very common in children’s stones, and struvite frequency rose in people over 80 years old.
4.7. Sex-related evolution of components
Our results highlighted significant differences in stone composition between women and men, especially for uric acids, COD and carbapatite. Although COM was the most common component for both gender, women’s stones contained more often carbapatite (51.6% versus 32.7% for men). This ranking was found to be similar to those in other countries [13, 15, 17]. COD stones were also related to gender and more present in men. Furthermore, the drop of COD frequency was also initiated at the age range of 16–25 years in women while it was delayed to the age of 26–40 years in men.
Lastly, the increase of uric acid stones started later in women (from range 61–80 years) compared to men (from range 41–60 years).
4.8. Randall’s plaque
Over the last five years, around 7.5% of COM-containing stones of our database were developed from Randall’s plaque. This prevalence is low compared to others countries [10, 20]. A large part of COM-containing stones were not intact when they arrived in our laboratory for analysis, which surely impaired RP’s detection. Accordingly, we observed an umbilication for only 11% of stones (data not shown) which probably reflects this stone fragmentation. We also did not systemically scratch the stone umbilication to identify a RP component when RP was not visible under binocular magnifier, which certainly also decreased our RP’s frequency.
Two different crystalline phases, carbapatite and sodium urates, were described with a predominance for calcium phosphate. Only men had sodium urate in Randall’s plaque, which may be linked to a high level of dietary salt consumption [21], as a “Swiss survey on salt intake” revealed that dietary salt intake in the Swiss population was clearly above the international recommendation of 5 g/day, and more markedly so in men than in women [22].
Finally, as observed by Letavernier et al. [20], patients who showed RP were significantly younger whatever the gender.
5. Conclusion
This report is a first picture of the chemical composition of stones and influence of age and gender over the last ten years in the west of Switzerland. Although it includes a rather large number of calculi for a relatively small country (8.5 million people), this study deserves further analysis on number of stones experienced by patients, details on stone composition at first episode associated with degree of recurrence, and patient comorbidities. These will be the topics of a future publication.
Conflicts of interest
Authors have no conflict of interest to declare.