

1 Introduction
Line bisection is a perceptual-motor task commonly used in neurological examinations for assessing hemispatial neglect. The task requires to localize and mark with a pencil the center of a line drawn on a sheet of paper. When patients with hemispatial neglect bisect horizontal lines, they place the subjective midpoint toward the ipsilesional side [1]. Neglect may occur along horizontal, radial, and vertical dimensions of space [2–4].
Bisection performance has been extensively studied also in healthy individuals. Several factors may influence their performance, such as spatial orientation [3,4], learned reading direction [5], presence of contextual stimuli [6–8], and the age of the subjects [9]. Some researchers found a tendency of healthy subjects to bisect horizontal lines to the left of the true midpoint [4], others reported considerable interindividual variability in the direction and extent of errors [10,11]. Conversely, a consistent bisection bias was reported for bisection of radial and vertical lines [3,12,13]. Healthy individuals tend to bisect radial lines farther than, and vertical lines above the true midpoint [3,12,13]. Shelton et al. [3] attributed this bias to perceptual/attentional factors. During visual exploration, attention is preferentially distributed away from the body (“far peripersonal space”), since the visual system is tuned to detect distant stimuli [3].
Experimental evidence suggests the existence of separate neural systems involved in shifting attention along radial and vertical space dimensions. Occipitoparietal areas would shift attention toward the near/lower space [2,14–17], occipitotemporal areas toward the far/upper space [3,14,18]. An important question is whether the shifting of attention along the radial and vertical dimensions of space depends on a single mechanism or on separate mechanisms. We tried to answer this question by asking a group of healthy participants to bisect radial and vertical lines. Our prediction was as follows:
- • the presence of a significant correlation between radial and vertical bisection errors would have supported the hypothesis that a single system was involved in producing the attentional bias directed toward far/upper space;
- • the absence of a significant correlation between radial and vertical bisection errors would have supported the hypothesis that separate systems were involved in producing the attentional bias directed toward far/upper space.
2 Materials and methods
2.1 Participants
Ninety healthy, right-handed subjects (70 women and 20 men) participated in the study. Their mean age was 21.8 years (SD 2.5, range 19–28). The Edinburgh Handedness Inventory [19] was used to measure handedness (mean score = 95.6, SD = 6.2, range = 85–100). The participants were students at the University of Campania “Luigi Vanvitelli”. They reported having normal or corrected-to-normal vision. The experiment was approved by the ethics committee and was performed in accordance with the 1964 Declaration of Helsinki. Participants gave written informed consent to take part in the study.
2.2 Stimuli
The stimuli were black lines 24 cm long and 1.0 mm wide. They were drawn and centered on a sheet of white paper 29.7 cm × 21.0 cm.
2.3 Procedure
The participants sat in a comfortable chair in front of a table where the stimuli were presented along the radial and vertical axes. Radial stimuli were presented on the table top, 45 cm below eye level, at the intersection of the transverse and midsagittal planes. Their midpoint was 35 cm from the participant's body. Vertical lines were presented on a wall, 35 cm front the participant, at the intersection of the frontal and midsagittal plane, and their midpoint was at the subject's eye level.
The experimenter presented the stimuli one at a time. The participants were asked to bisect the lines using a pencil held with their right hand. Each participant bisected a total of 20 lines, administered in two blocks of trials [(radial vs. vertical axis) × ten presentations]. In each block, the lines were presented in either the radial or the vertical axis, and the order of the two blocks was counterbalanced across subjects. Line bisection error (LBE) corresponded to the distance of the subjective midpoint from the true center. It was measured to an accuracy of 0.5 mm. Deviations farther than (radial lines), or above (vertical lines) the true center were assigned a positive value, whereas errors nearer than, or below the true center were given negative values. The standard deviation of the LBE, calculated for each condition, was the variable bisection error (VBE). Variability scores quantify the scatter of subjective midpoints and are sensitive to variability or inconsistency in responding.
2.4 Statistical analysis
The mean values of LBE and VBE were analyzed. They were subjected to one-way analyses of variance with axis (radial vs. vertical) as the within-subjects factor. Furthermore, to investigate the direction of misbisection in each axis condition, one-sample, two-tailed t tests (df = 89) were also performed comparing LBE with the null set (true center). Significance level was fixed at p = 0.025, considering an overall 0.05 level divided by the number of comparisons, according to Bonferroni procedure. Finally, to investigate whether there was a relationship between radial and vertical LBEs, we calculated the Pearson correlation coefficient between the two variables.
3 Results
The mean values of LBE and VBE are graphically reported in Fig. 1a and b, respectively. The axis significantly influenced LBE (F(1,89) = 43.65, p < 0.0001; radial axis = 3.89 mm; vertical axis = 7.49 mm). One-sample, two-tailed t tests (df = 89) showed that subjects bisected radial lines farther than, and vertical lines above the true midpoint (radial axis: t = 8.09; p < 0.0001; vertical axis: t = 13.39; P < 0.0001). No significant axis effect was found on VBE (F(1,89) = 3.42, p = 0.07; radial axis = 4.12 mm; vertical axis = 3.77 mm).
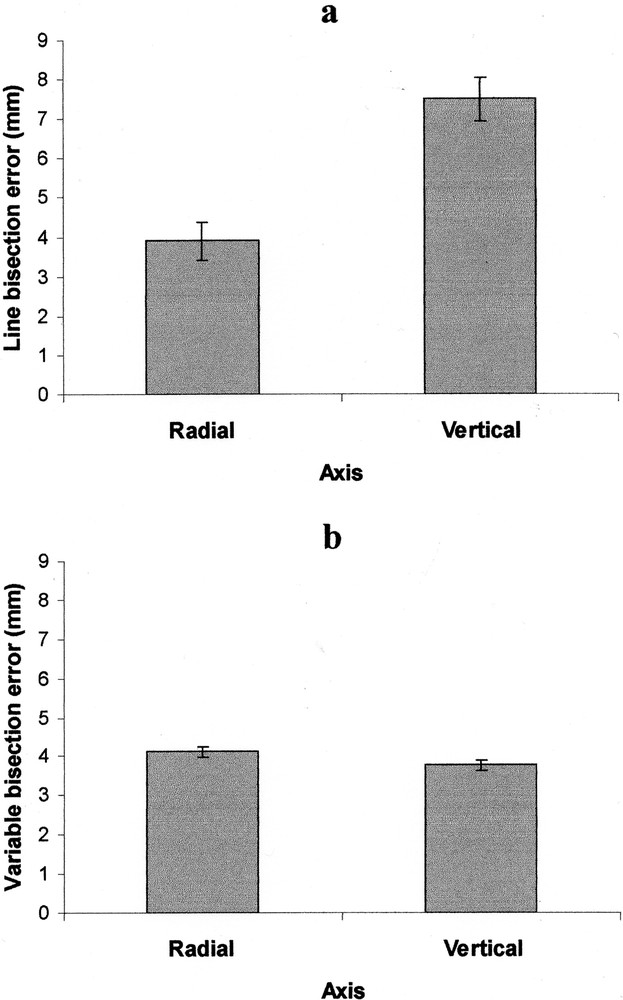
Mean values of line bisection errors (a) and variable bisection errors (b) in radial and vertical axis conditions. Positive values of line bisection errors indicate that misbisection was farther than (radial condition) or above (vertical condition) the true center. Error bars indicate SE.
Finally, a significant positive correlation between radial and vertical errors was observed (r = 0.46, t = 4.86, df = 88, p < 0.0001).
4 Discussion
The main findings of the present study were:
- • participants bisected radial lines farther than, and vertical lines above the true centre. This result is in line with previous studies [3,12,13]. However, the bisection bias in the vertical condition was greater than that in the radial condition. Interestingly, VBE did not differ between the two spatial conditions. Variable scores quantify the scatter of subjective midpoints and are sensitive to variability or inconsistency in responding. Therefore, in our experiment, the consistency of bisection performance was similar in the radial and vertical conditions;
- • a significant positive correlation between radial and vertical LBEs was present. This observation support the hypothesis that a single neural mechanism was involved in producing attentional bias directed toward far/upper space.
As mentioned above, experimental evidence suggests the existence of separate attentional systems involved in shifting attention toward far/upper vs. near/lower space [14]. The occipitoparietal (dorsal) system would shift attention toward near/lower space, occipitotemporal (ventral) system toward far/upper space [2,3,15–18]. Drain and Reuter-Lorenz [14] suggested that the two systems are in mutually inhibitory control of attention orienting. Damage to occipitoparietal regions would lead to a concomitant disinhibition in occipitotemporal activity and a far/upward orienting bias. Conversely, occipitotemporal damage would produce a disinhibition in occipitoparietal activity and a near/downward orienting bias [14]. Then, it is possible that the bisection biases observed in healthy individuals might depend on an imbalance between neural attentional mechanisms. In other words, occipitotemporal activity that shifts attention toward far/upper space would prevail over occipitoparietal activity that shifts attention toward near/lower space. Note that when the participants foveated the central region of the line to localize the subjective midpoint [20], the images of the distal (radial lines) and upper (vertical lines) portions of the line was projected onto the inferior retina (and processed primarily by the occipitotemporal stream), and the images of the proximal (radial lines) and lower (vertical lines) portions onto the superior retina (and processed primarily by the occipitoparietal stream). This might have magnified the magnitude of the distal and upper portion of the line. Previous studies showed that the magnitude of attended stimuli appears magnified compared to that of unattended stimuli [21–24]. In this way, the magnification of the distal (radial lines) and upper (vertical lines) portion of the line might have moved forward and upward the location of the subjective midpoint, respectively.
An important issue that has been addressed in the present study was whether the attentional bias toward far/upper space depended on a single mechanism or on separate mechanisms. To answer this question, we examined whether there was a relationship between radial and vertical bisection errors. Our results showed that a significant correlation between the errors in the two spatial dimensions was present. This observation supports the hypothesis that a single mechanism, depending on the activity of occipitotemporal stream, is involved in shifting attention toward far/upper space.
In favor of this hypothesis, there are some neurological observations. Shelton et al. [3] reported a patient with far radial and upper vertical neglect. The patient presented ischemic lesions involving both occipital and inferior temporal lobes.
Shelton et al. [3] asked the patient to bisect visually presented lines and wooden rods while blindfolded. They observed that the patient bisected radial lines (and rods) nearer than, and vertical lines (and rods) below the subjective midpoint of the control group. A completely opposite behavior was observed by Mennemeier et al. [16] in a patient with bilateral posterior parietal lobe, and near/lower neglect. The patient localized the midpoint of visually presented lines and wooden dowels, while blindfolded, farther than and above the subjective midpoint of the control group [16].
In conclusion, both our observations on healthy individuals and previous observations on brain-damaged patients [3,16] suggest that a single neural mechanism is involved in shifting attention toward far/upper space.